EQUINE JOINT THERAPY

The field of equine arthrotherapy is constantly changing due to intensive ongoing research and the regular release of innovative new products.
This article highlights the more common strategies currently used to treat joint disease in the horse.

Regardless of the joint(s) involved, our therapeutic goals are the same:
• To modify the symptoms by reducing pain and lameness, and
• To modify the disease by discouraging progression of joint deterioration.
Learn How Equine Joints Live |
|
 |
Learn About NORMAL Joint Physiology HERE. |
 |
Learn About ABNORMAL Joint Physiology HERE. |
I. CORRECTIVE SHOEING
In most cases, we can trim and shoe the horse in a way that minimizes challenge to affected joint(s). Our goal is to make the arthritic joint work as little as possible while still maintaining normal overall movement and function. In order to do this, we have to optimize the way the joint moves and bears weight during exercise. Corrective shoeing can counteract some of the abnormalities that contribute to joint instability.
We frequently manipulate joint movement and weightbearing by implementing one or more of the following techniques:
• Facilitating breakover. Easing breakover often decreases the degree of flexion and extension the joint undergoes during exercise. For the most part, less movement of this type reduces the joint's predisposition to instability. Less instability results in less inflammation and improved overall comfort.
• Normalizing joint angle. Arthritic joints often have abnormal angles relative to the rest of the limb. Joint angles can be altered from front-to-back and/or from side-to-side. Minimizing these alterations can enhance joint stability and improve comfort.
• Equalizing joint pressure. Most joints are designed to bear weight uniformly across the entire articular surface. Abnormal joint balance and/ or limb movement can alter these forces, resulting in excessive compression on one side of the joint and tension on the other. Normalizing pressure across the joint surface discourages abnormal wear of the articular cartilage.
• Reducing joint compression. Excessive compression across the articular surface can affect the metabolism and wear of the articular cartilage. Lighter horses, for instance, are less predisposed to joint problems as to compared to heavier horses.
• Maintaining normal motion characteristics of the joint. The joint is happiest when the flight path of the limb is straight and the limb is directly in line with its center of gravity. The position of the limb both on the ground and in the air can be manipulated via shoeing.
II. SYSTEMIC ARTHROTHERAPY
Several advancements have been made in the field of systemic joint therapy over the last decade. We will review a few of these strategies.
Any medication administered outside the joint (by mouth, intravenously, or intramuscularly for example) for the purpose of improving joint function and/or comfort is considered a form of systemic arthrotherapy. Anti-inflammatory medications (such as phenylbutazone and Banamine), topical pain relievers (such as capsaicin and diclofenac), and joint supplements (such as Adequan®, Legend®, and Cosequin®) are included in this category.
Joint supplements have seen wide use in recent years, and are most often the client's first line of treatment for DJD in their horse(s). The primary goal of the joint supplement is to stimulate normal activity and function of the synovial membrane thereby enhancing the integrity of the joint environment. Topical, oral, intravenous, and intramuscular forms exist.
A. Non-Steroidal AntiInflammatory Drugs (NSAIDs)
Non-steroidal antiinflammatory drugs (NSAIDs) such as Bute, Banamine, Ketofen, etc.) are frequently used to alleviate the clinical signs (namely inflammation and pain) associated with arthritis in horses. However, consistent use can result in gastric ulceration as well as kidney and liver dysfunction. Therefore, we recommend this form of therapy only for horses that perform very infrequently, such as once or twice weekly (or less).
Firocoxib is a NSAID that has been shown to reduce inflammation and pain associated with osteoarthritis in horses. At the same time, it offers a much better safety profile when compared to other (more traditional) NSAIDs. Equioxx® is the first coxib class nonsteroidal antiinflammatory drug that is highly selective against Cyclooxygenase-2 (Cox-2) prostaglandins which are responsible for inflammation. Unlike other NSAIDs, however, Equioxx® spares the beneficial Cox-1 prostaglandins required for normal gastric, renal (kidney), and hepatic (liver) function. A single dose lasts for 24 hours and can be administered for up to 14 days in a row.

Surpass® (diclofenac sodium) is a topical medication that has gained popularity due to its ease of administration (simply rub it on the affected joint) and its effectiveness for certain types of arthritis in horses. In our experience, Surpass generally works better under the following circumstances:
• In higher-motion joints. For example, we would expect a better response when treating a fetlock joint (which is very high-motion in nature) than we would when treating the lower hock joints (which are very low-motion in nature).
• In joints that are closer to the skin surface. If there is less tissue through which the product is required to diffuse then more will be delivered to the affected area. Consequently, we would anticipate a better clinical response if more product is reaching the joint. For example, we would expect a better response when treating a fetlock joint (which is just under the skin surface) than we would a stifle joint (which is much further/ deeper from the skin surface).
• In joints with a high topical surface area:size ratio. We typically observe a higher concentration of therapeutic medication in synovial (joint) tissue (and therefore a better clinical response) when the joint is smaller and very well exposed under the skin surface. For example, we would expect a better response when treating a fetlock joint (small and just under the skin surface) than we would a stifle joint (large and deep under the skin surface).
• When used prophylactically (as a preventative) rather than subsequent to the onset of joint inflammation. In other words, we would expect a better response if we applied the product prior to exercising the horse than we would if we applied the product after we finished riding.
B. Oral Joint Therapies (i.e. Given by Mouth)
Most studies show that the oral medications (e.g. Cosequin®, MSM, Flex Free®, Corta-flex®, etc.) are quite effective when absorbed into the system. This type of arthrotherapy works especially well in people and dogs, who are able to absorb relatively large molecules (like glucosamine and chondroitin sulfate) through their intestinal wall easily. Horses, on the other hand, are generally not proficient at absorbing large molecules into their system from the intestinal tract. Therefore, a portion of the oral medication (and the client's investment) may not be completely utilized. Many companies are continually working to find ways to improve absorbability of oral supplements in the horse.
C. Injectable Joint Therapies (i.e. Given in the Muscle or Vein)
Medications which bypass the intestinal tract of horses (and therefore do not rely on intestinal absorption) are generally preferred due to their respective molecular availabilities. These are injectable (i.e. given as a shot) and include both LONG-TERM (maintenance) and SHORT-TERM forms.
SHORT-TERM medications are administered intravenously (IV) and therefore typically have a greater positive effect on joints. In other words, we generally observe more improvement in the horse's comfort following administration of short-term therapy (such as Legend®) than we do following administration of long-term therapy (such as Adequan®). The positive effect of short-term therapy, however, is only about one-half as long as that of long-term therapy.
It is for this reason that we recommend short-term therapy and long-term therapy with different goals in mind.
We currently recommend LONG-TERM joint therapy in the following instances:
• In horses with no current evidence of joint disease. In this case, the purpose of the medication is to delay the onset of joint disease.
• In horses with mild joint disease. In this case, the purpose of the medication is to alleviate symptoms enough for the horse to perform well in his/her intended capacity.
• In horses with moderate to severe joint disease that have previously been treated with local therapy (i.e. injection). The purpose of the medication in this case is to prolong the effect of the injection and delay the recurrence of clinical signs.
Long-term/ maintenance medications include Adequan®, Acetylglucosamine, Ichon™, Chondroprotec®, Pentosan and Glucosamine (among others). Most treatment protocols involve one injection (approximately 5cc or 500mg) in the muscle once weekly for 4 consecutive weeks and then continuing administration once or twice monthly thereafter (indefinitely). Luitpold (the maker of Adequan®) suggests administering a dose of their product once every 4 days for 7 treatments and repeating this protocol bi-annually. Cost for these products may vary between $12 to $50 or more per dose.
Learn How to Properly Administer an Intramuscular (IM) Injection |
|
 |
Click HERE to watch the video tutorial. |
 |
Click HERE to see our written recommendations. |
We currently recommend SHORT-TERM joint therapy 36-48 hours prior to a race, clinic, or show. The purpose of the medication is to maximize the performance of the horse for a selected event.
Short-term medications include Legend®, MAP-5, and Polyglycan® (among others). These medications are generally administered intravenously (in the vein) at varying doses. The cost of a single dose can range from $35 to $95.
If regular short-term treatment (i.e. an IV dose administered every 2-4 weeks or sooner) is required to produce and/or maintain soundness or does not result in a satisfactory response, then local arthrotherapy (i.e. joint injection) may be considered (see below).
D. Biphosphonate Therapy
Biphosphonates are a class of drug formulated to reestablish normal bone metabolism in pathologic conditions. They have a tremendous affinity for hydroxyappetite (a basic building block of bone) and work by inhibiting osteoclast-mediated bone resorption. This is accomplished by altering the metabolism of osteoclastic cells, thereby resulting in their death. Osteoblastic cells are then able to more effectively improve bone density and strength in an environment absent of osteoclastic activity.
In addition to hindering osteoclastic resorption of bone, biphosphonates may also function to dampen the response of chemical mediators involved in the process of inflammation. Both anti-inflammatory and analgesic (pain-relieving) properties have been suggested, although further research is needed to confirm this argument.
It should be noted that there are several explicit contraindications relating to the use of biphosphonates in horses. These should be reviewed carefully prior to considering this form of therapy for your horse.
At The Atlanta Equine Clinic, the use of biphosphonates has proved beneficial in cases of navicular inflammation, nonadaptive bone remodeling, and chronic severe osteoarthritis. TILDREN® (tiludronate) and OSPHOS® (clodronate) are two products frequently implemented in our practice.
Tildren® inhibits excessive bone resorption and promotes rebalancing of bone metabolism.
Osphos® is an injectable bisphosphonate solution which implements a similar mode-of-action as Tildren® by discouraging bone resorption by binding to calcium phosphate crystals (inhibiting their formation and dissolution) and by exerting direct cellular effects on osteoclasts. Unlike Tildren®, however, Osphos® has the unique advantage of intramuscular injection and is a ready-to-use solution that does not require mixing or reconstitution. It is also considerably less expensive than Tildren®.
III. LOCAL ARTHROTHERAPY (JOINT INJECTION)
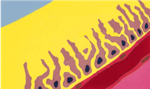
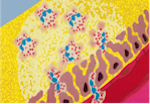
Joint injection enables us to deliver high concentrations of therapeutic medication directly to the synovial membrane of the affected joint(s). The synovial membrane is responsible for producing hyaluronan (hyaluronic acid/HA) which is responsible for lubricating and protecting the articular cartilage. The synovial membrane is also responsible for the release of inflammatory cells in compromised joints.
A. Corticosteroids
When performing joint injection, veterinarians often elect to infuse a combination of synthetic hyaluronan and corticosteroid. Steroids effectively eliminate inflammation within the affected joint while hyaluronan serves to reestablish a normal synovial environment.
Many horse owners are concerned about the effects that corticosteroids will have in their horse's joint(s). This concern is primarily a consequence of reports of accelerated joint deterioration pursuant to the abusive use of steroids in racehorses.
There is no question that corticosteroids can have deleterious effects in the equine joint. However, we should consider the whole picture when considering its use in the performance horse: |
|
Let's say we don't infuse steroid into the joint. The inflammatory cells will persist in the joint. As a result, the following consequences will occur: • The presence of the inflammatory cells within the joint will increase the hydrostatic pressure within the joint causing the influx of fluid. Increased synovial fluid in the joint (called effusion) results in stretching of the joint capsule (which houses nerve endings) and pain. So lameness will persist. • The inflammatory cells release degradative enzymes (called lysozymes) and other chemical mediators that break down hyaluronan (HA) within the synovial fluid. The fluid becomes very thin and watery, thereby losing its ability to protect the cartilage. Consequently, we get erosion of the cartilage which in turn results in increased joint instability, inflammation, and so on. In other words, persistent inflammation is not healthy for a joint! |
|
Let's say we infuse steroid into the joint: • The presence of steroid will reduce inflammation within the synovial environment. As a result, the hydrostatic pressure will decrease, fluid will leave, the joint will decompress, and will be more comfortable. Furthermore, there will be less degradation within the joint due to the absence of the inflammatory enzymes and mediators. Therefore, in one sense, steroids are helping us to improve synovial integrity. • On the other hand steroids also result in breakdown of HA which, as we previously discussed, is chondroprotective (protects the cartilage). Therefore, we must weigh both sides when considering the use of steroids in equine joints. |
|
The factors that determine if intraarticular steroid injection is appropriate for a specific case of lameness include:
• How important is the integrity of this joint in regard to the soundness of the horse Is it a high motion joint Is it a highly weight-bearing joint?
The thoracic (front) fetlock is one of the most important (i.e. clinically-significant) joints in the horse. Per unit area, it is the highest-motion and bears the greatest amount of weight when compared to other joints. This joint must be comfortable and have a normal range-of-motion for the horse to be sound. When treating this joint, we should do it in a way that promotes long-term synovial integrity and health.
The distal hock joints, on the other hand, are not very important (i.e. not clinically-significant). They move very little during exercise, and as a result are not essential for normal locomotion of the limb. In fact, if the horse did not have these joints (i.e. if there was solid bone in place of the joints) we would not be able to detect an appreciable gait abnormaility. Accordingly, we sometimes elect to surgically or chemically fuse these joints in horses that are refractory to other forms of therapy. Veterinarians, therefore, have the luxury of being quite aggressive in regard to therapeutic strategy without the concern of imposing deleterious side effects. When it comes to the lower hock joints, our primary focus is not maintaining good synovial integrity but rather keeping the horse comfortable and sound. It is for this reason that hock injections are far more common than most other types of joint injection.
• How much inflammation is present in the joint?
Inflammatory changes can eventually become irreversible. This leads to greater joint disease and further inflammation. The deleterious effects of inflammation may outweigh those that occur pursuant to steroid injection. In many cases of joint disease, intraarticular steroids are healthier for the joint than a lack of steroids. In other words, the benefit of steroids sometimes outweighs its deleterious side effects.
B. Adequan I.A. (Polysulfated Glycosaminoglycan)
Adequan obtained the approval of the Food and Drug Administration (FDA) for intraarticular injection in 1984. It is the only joint therapy clinically proven to relieve symptoms associated with arthritis and treat the underlying causes of equine non-infectious degenerative joint disease. Studies suggest that Adequan IA may potentiate joint infection, however, which is a rare but potentially life threatening complication.
To reduce the likelihood of complication, most veterinarians infuse Adequan IA in combination with antibiotic (usually amikacin) into the joint. Although this approach dramatically decreases the risk of developing post-treatment septic arthritis (joint infection), the co-infusion of amino glycoside antimicrobials (such as Amikacin) can precipitate synovial irritation. Amikacin has been shown to be cytotoxic to to equine joint cells and mesenchymal stromal cells (MSCs). Therefore, the addition of antibiotic to the treatment regimen may actually diminish the positive effect of the treatment.
It should be noted that there is no correlation between administration of Adequan IM (the intramuscular form) and septic arthritis (joint infection). We frequently implement Adequan IM as part of our long-term arthrotherapeutic strategy (see above).
C. Legend (Hyaluronate Sodium)
Legend is the only FDA approved intravenous and intraarticular therapy designed to treat equine non-infectious synovitis associated with osteoarthritis. It is a preparation of pure hyaluronate sodium, the same glycosaminoglycan present in normal joint fluid. Legend is produced by a patented biofermentation process, resulting in such purity that it can be given intravenously for immediate bioavailability.
We have observed excellent results when using Legend intravenously in our practice. The effect of IV injection peaks in about 48 hours and lasts for approximately 2 weeks.
D. MAP-5 (Hyaluronate Sodium)
MAP-5 is a patented salt of hyaluronic acid in normal saline for use in the collection, handling, culture and cryopreservation of embryo, ova, sperm and other cells. Although this product is licensed for use as a cryopreservative, it has proven to be very effective as an off-label treatment for equine arthritis.
We often recommend MAP-5 for IV use in place of Legend, as it seems to have a comparable effect and is considerably less expensive. It can be administered both intravenously and intraarticularly.
E. Polyglycan
Polyglycan is a highly viscous aqueous solution of defined fractions of purified Hyaluronic acid, Chondroitin sulfates A-and-C in a 10% solution of N-acetyl-D-glucosamine. Some clients consider this product to be a combination of Adequan and Legend; this is not exactly accurate, although Polyglycan does contain components that are representative of both.
Polyglycan was initially developed as a post surgical joint lavage with the goal of quickly reestablishing synovial physiology following arthroscopic or arthrotomic surgery. Polyglycan contains naturally occurring components of synovia that play a central role in maintaining the homeostatic environment of the joint.
Soon after it's introduction into the equine market, however, off-label intraarticular and intravenous applications quickly popularized. In our experience, Polyglycan has comparable benefit to Legend with respect to both intravenous and intraarticular administration. Some clients think that it works better than Legend when administered intravenously (IV), although this comprises the minority of opinions.
We do implement Polyglycan intraarticularly for post-surgical cases, although typically elect to use high-vicosity hyaluronan (i.e. Hylartin or Hivisc) as part of our intraarticular protocol in horses with chronic joint disease.
Several lay-people (not our clients) have complained of excessive hemorrhage/ bleeding as a result of Polyglycan administration, although these reports are highly-speculative and there have been no clinical observations to this effect.
F. Pentosan Polysulfate (PPS)
Pentosan is a linear polymer prepared from xylan, a complex hemicellulose extract of plant (Beechwood) origin. PPS is one of the sulfated heparinoid compounds. The heparin-like anti-coagulant effects have been reduced and the anti-inflammatory, fibrinolytic, and tissue trophic effects have been enhanced. It is administered both intramuscularly (IM) and intraarticularly (IA) in the horse.
In addition to promoting synovial intergrity and inhibiting enzymal degradation of the joint, Pentosan may have increased antiinflammatory effect as compared to other products. This quality may obviate the need for concurrent use of intraarticular corticosteroids, upon which which many veterinarians rely for their potent antiinflammatory properties. The potential deleterious effects of intraarticular corticosteroids on articular cartilage have been well-documented (see above).
In our experience, intraarticular Pentosan alone does not produce a positive clinical effect beyond that of a hyaluronan/steroid combination. The antiinflammatory effects of corticosteroid appear to be much stronger. This observation coupled with our current ability to use relatively safe (non-deleterious) articular steroids (such as Betamethasone) usually prompts us to implement a hyaluronan/ steroid combination during our initial treatment of equine arthritis.
Subjective opinions of intraarticular Pentosan vary considerably among our clients. Some think that is makes a tremendous difference in their horse's performance; others do not observe any positive effect. Lack of effect may occur in lieu of the recommended dose of 3mg/kg being inadequate (too low). It is for this reason that we typically offer Pentosan as a second-line strategy to our clients that are willing to try it.
We should note that if a combination of hyaluronan and steroid has already been implemented unsuccessfully, it is unlikely that intraarticular Pentosan will prove to be effective.
G. Polyacrylamide Hydrogel (PAAG)
Polyacrylamide hydrogel is a nondegradable synthetic viscous gel that has been shown to decrease symptoms associated with knee arthritis in human patients. PAAG is an atoxic, stable, nonresorbable sterile watery gel consisting of approximately 2.5% cross-linked polyacrylamide and nonpyrogenic water. In addition to treating knee arthritis, PAAG has been widely used in ophthalmic operations, drug treatment, food packaging products, and water purification.
Polyacrylamide hydrogel has also proven to be an effective synthetic joint lubricant for horses. Its long-term effects make it a viable treatment for horses with chronic degenerative joint disease. To date, no adverse effects pursuant to its use have been reported.
H. Autologous Conditioned Serum (ACS)
The exploration of interleukin-1 receptor antagonist protein (IL-1Ra or IRAP) as a treatment for synovitis, osteoarthritis and rheumatoid arthritis began shortly after its first published characterization in 1984. The ability of this molecule to act as both a symptom- and disease-modifying agent in various species (including horses and humans) has prompted its clinical application as a treatment for joint disease. The goal behind IRAP treatment is to use the body's own inflammation-fighting cells to reduce arthritis rather than the synthetically-produced antiinflammatory medications that we buy in a bottle. Because antiinflammatory cells are produced by the host body itself, we can often expect a greater degree and longer duration of response.
Autologous versus Allogeneic |
I. Mesenchymal Stem Cells (MSC)
Stem cells are receiving a great deal of scientific attention as well as coverage in the lay press. The primary reason for the attention is the potential ability of stem cells to regenerate tissues without the production of scar tissue that is generally associated with healing processes. The goal through stem cell use, therefore, is to replace damaged tissue with something comparable to the original tissue rather than with scar tissue.
At The Atlanta Equine Clinic, we typically reserve stem cell use for those joints with subchondral lesions (affecting the underlying bone).
J. Platelet-Rich Plasma (PRP)
Numerous growth factors have been used in the horse with the intention of enhancing synthesis and reducing breakdown of tendon/ ligament tissue pursuant to injury. Such growth factors can been harvested from bone marrow and/or fat aspirates, which also contain increased concentrations of stem cells.
Platelet-Rich plasma (PRP) is another viable source of growth factors that augment equine tissue repair. (PRP) is an autologous concentration of platelets in a small volume of plasma. Plasma is the straw-colored liquid in which blood cells are suspended. PRP is generated through relatively simple centrifugation of blood. Because it is a concentration of platelets, it is also a concentration of 7 fundamental protein growth factors known to be secreted by platelets in response to wound healing. PRP also contains proteins known to promote cell adhesion during tissue rebuilding.
Platelets perform many functions in the body, including formation of blood clots and release of growth factors into wounds. The rationale for the use of PRP as a treatment strategy for tendonitis (tendon damage) and desmitis (ligament damage) stems from the increased platelet release of multiple growth factors in response to an injury. Two additional incentives for using PRP include its relative ease of collection and the unlikelihood that it will result in immune rejection since it is autologous (produced from the patient's own blood).
At The Atlanta Equine Clinic, PRP has been used to successfully treat the following soft tissue injuries:
• Tendon Strain
• Muscle Strain
• Ligament Strain
• Joint Capsular Laxity
PRP has also been used to treat intraarticular injuries. Examples include arthritis, arthrofibrosis, articular cartilage defects, meniscal injury, and chronic synovitis (joint inflammation).
K. Pro-Stride®
Pro-Stride® combines the positive effects of IRAP and PRP for use in damaged tissue (such as ligaments and tendons) and synovial structures (such as joints, tendons sheaths and bursas). It has become an effective weapon against progressive equine osteoarthritis in our practice.
By acting to restore the balance of inflammatory and anti-inflammatory cytokines, Pro-Stride® not only provides pain relief but also promotes regeneration of tissues within affected joints, thereby improving the horse’s prognosis for future performance (in the long-term). At The Atlanta Equine Clinic, Pro-Stride® therapy is often implemented in high-motion (i.e. clinically-significant) joints to reduce pain, improve function, and promote regeneration of damaged tissues. By using Pro-Stride®, we can avoid the deleterious effects imposed on cartilage by intraarticular corticosteroids (i.e. standard steroid injection) when appropriate.
Like PRP and IRAP, Pro-Stride® is an autologous product. It is produced in about 25 minutes using stall-side using a kit supplied by the manufacturer.
IV. SURGERY
Diagnostic and Surgical Arthroscopy allows for direct visualization of the joint's interior. In many cases, abnormalities not readily visible radiographically (upon x-ray) or ultrasonographically will be apparent through an arthroscope. Once isolated, certain lesions (such as meniscal tears, bone chips or subchondral cysts) can be debrided under arthroscopic guidance. "Cleaning up" the joint in this fashion may help to reestablish the horse's soundness. Diagnostic/ surgical arthroscopy may require general anesthesia, however, and therefore must be performed within a hospital environment. Cost for the procedure varies depending on the type and location of lesion(s).